The future of our healthcare system is in our hands; we approach it with responsibility, collaboration and a deep commitment to the well-being of all people. (Waldo Swiegers/Bloomberg via Getty Images)
South Africa’s healthcare system is failing, but experts say that this has less to do with an insufficient budget than the government’s poor use of its resources, bad management, corruption and patronage.
The same experts warn that the government’s National Health Insurance (NHI), estimated to cost between R300 billion to R500 billion annually, is not the panacea that will fix the systemic problems in the beleaguered healthcare system.
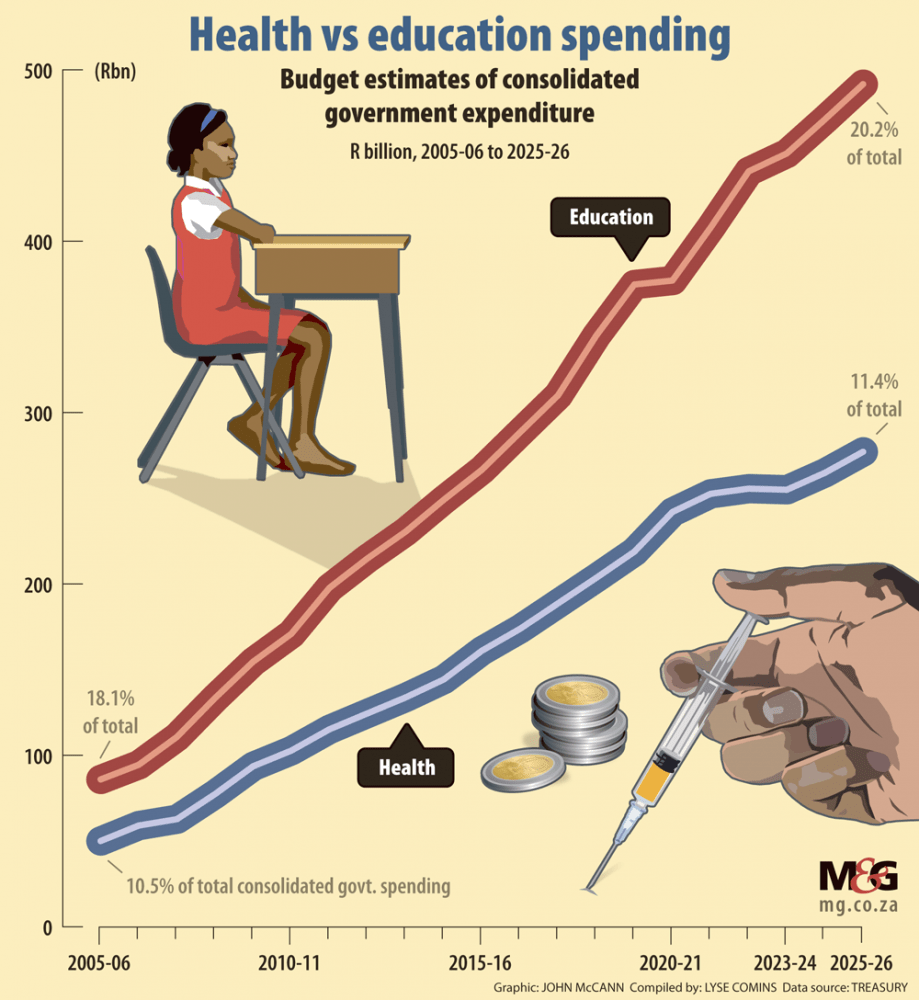
According to the treasury’s latest budget figures, spending on health has increased from just over R50 billion in 2005 to R254.9 billion in the 2023-24 financial year and currently represents 11.4% of the overall budget. The treasury’s estimated health budget will increase to R264.8 billion by 2024-25 and to about R277 billion in 2025-26, staying at 14.4% of the total budget over those two financial years.
Experts asked to analyse health spending and performance said that although the government had made significant progress in extending healthcare services to all citizens, the system is in need of a total overhaul — from who gets appointed as senior managers to balancing allocation of spending on supplies versus salaries.
LISTEN: The Fiscal Cliff | The jaws of the hippopotamus
While some experts contend that the health budget is big enough, research shows that spending on this vital line item has stagnated in real terms. Cutbacks have been intensified since the pandemic. In the second episode of our podcast series, the Mail & Guardian talks to the spokesperson of the Democratic Nursing Organisation of South Africa about how healthcare workers are feeling the spending pinch.
Alex van den Heever, of the Wits school of governance, said the government has largely failed to take advantage of the foundations of the health system that existed in 1994 to build one capable of addressing the needs of the entire population.
“Government has failed to introduce a coherent governance regime for the public system to ensure that it operates in the interests of users.
“Equally, it has failed to establish a regulatory framework that allows the private health system to operate more efficiently and fairly.”
These issues have been addressed in various committees of inquiry, he added, but the government had not come to the party.
Van den Heever blamed a system of patronage, which became more pronounced from the early 2000s, for dragging the health service down.
“Political actors, therefore, no longer focus on the public interest as their primary interest. As a consequence the quality of policy development and implementation has fallen to an all-time low — ensuring that the government cannot address complex social problems anymore.”
The health sector gets a good portion of the overall budget, Van den Heever said, adding that there is no reason to expand it further in the absence of strong economic growth.
The economy’s meagre growth — attributed to the government failures on the energy and logistics front — has severe implications for the expansion of the public health system, he said. “South Africa should be growing at around 3% to 4% per annum on a permanent basis. Unfortunately, due to government failures, we are not able to grow faster than around 1% per annum — at best.”
Despite a growing budget, research by the University of the Witwatersrand’s Public Economy Project (PEP) shows that healthcare budgets have come under increasing pressure. The PEP said healthcare expenditure has stagnated in real terms relative to the population dependent on government services.
In 2012, there were more than 720 healthcare workers per 100 000 uninsured people. This ratio has steadily fallen since then, reaching 632 by 2018.
Spending cutbacks have been intensified since the Covid-19 pandemic, the PEP noted, with pay increases for government workers held below the rate of inflation, and across-the-board spending reductions cutting deeply into healthcare.
Van den Heever acknowledged that there can never be enough money to meet the country’s health needs, but said this predicament makes it vital for services to be planned and managed efficiently and fairly to maximise the use of resources. There are about 310 000 employees in the sector, which he said was “substantial”.
“At present, vast portions of the health budget are wasted through improper procurement and poor appointments. The present allocation, which amounts to roughly 4% of GDP, is generous in comparison to other peer countries. But the allocations are used so poorly that we have some of the worst health outcomes for a country of our level of development,” he said.
But Van den Heever believes the public sector has the “latent capability” to deliver a comprehensive range of high-quality primary care and hospital-based services.
 (John McCann/M&G)
(John McCann/M&G)
“We are, however, not able to do this consistently throughout the entire country — largely due to governance failures at all levels of the system,” he said.
“A new governance framework is required that results in merit-based appointments and a focus on service delivery. The first step in this is to design frameworks that remove the ability of political appointees to appoint and remove people in both the administrations and services.”
Critical of the NHI, he said the plan fails to confront the shortcomings of the health system and “appears designed to reinforce the systems of patronage that have undermined performance throughout the public sector, including the health system”.
“The NHI is largely a distraction from the real reforms that should be considered. There has been no systemic reform since 2003. The NHI is a cynical distraction to avoid having to properly account for years of policy neglect,” he said.
Susan Cleary, the director of the University of Cape Town’s School
of Public Health, said the government had done well since 1994 to develop a “unified public healthcare system that caters to the majority of the population under the management of provincial departments of health”.
There had been real per capita increases in the budget for the public healthcare sector and important improvements such as largely free services, Cleary said. But the sector is hamstrung by corruption, while resources are poorly managed.
“At this stage our wage bill is starting to crowd out our spending on supplies, which is terribly inefficient. Health workers might be in the clinics and hospitals but have no supplies or other tools of their trade,” she said.
Rural Health Advocacy Project director Russell Rensburg said the post-apartheid government had invested significantly in primary healthcare, built or refurbished more than 1 600 health facilities and introduced free primary healthcare services.
The country had done well in addressing the HIV/Aids crisis since 2002, with 90% of people living with HIV knowing their status, 77% on treatment and more than 90% of those on treatment virally suppressed, Rensburg said. Moreover, reproductive maternal and child health has improved and maternal mortality at a national level is trending down, while under-five mortality has also decreased. Much of this can be attributed to the introduction of antiretroviral therapy, he said.
But, Rensburg noted, the population’s health status is also determined by social conditions such as adequate housing, levels of education and income.
On the issue of the NHI, Rensburg said it is not “the panacea” to all problems in the sector.
In the short term the NHI could provide an enabling framework to improve publicly funded services by segmenting the health system into district health services, providing autonomy for hospitals and ensuring services are standardised across districts, he said.
“It also allows for improved accountability at all levels of the health system as well as reducing the political interference prevalent in most provincial administrations.”
The government needs to invest in health management information systems to strengthen governance and decision-making, while also improving the leadership capacity of hospital management and boards, Rensburg added.
“The current system of spending is not informed by need or effective use of resources; rather we allocate funding based on historical allocations.”
Rensburg said South Africa’s goal should be to improve the health of all people and ensure equitable access to the health services they need.
“For example we offer a comprehensive package of services in the public sector including advanced cancer care. But we don’t know if we are reaching all the people in need of cancer care — better data will assist in answering these questions as well as improving efficiency and equity.”
This article forms part of the second instalment of The Fiscal Cliff, a monthly series by the Mail & Guardian on the state of South Africa’s public purse. The series looks into the effect of fiscal consolidation on public services — which have steadily deteriorated over the years — and considers this policy’s impact on the country’s growth prospects. You can read the other article in part one of the series here.