A Male nurse assists one of the injured initiates at St Barnabas Hospital in Mthatha, South Africa. (Photo by Gallo Images / City Press / Leon Sadiki)
Many years ago, a friend repatriated her family to Europe because her son needed intricate surgery. When an African leader learnt of this, he wrote to her and offered financial help. She declined, reminding him that in France healthcare is free for all.
The president in question is no longer in power and her son is now a young adult. South Africa still does not have universal healthcare, which the World Health Organisation defines as everybody having access to the full range of quality health services they need, when and where needed, without financial hardship.
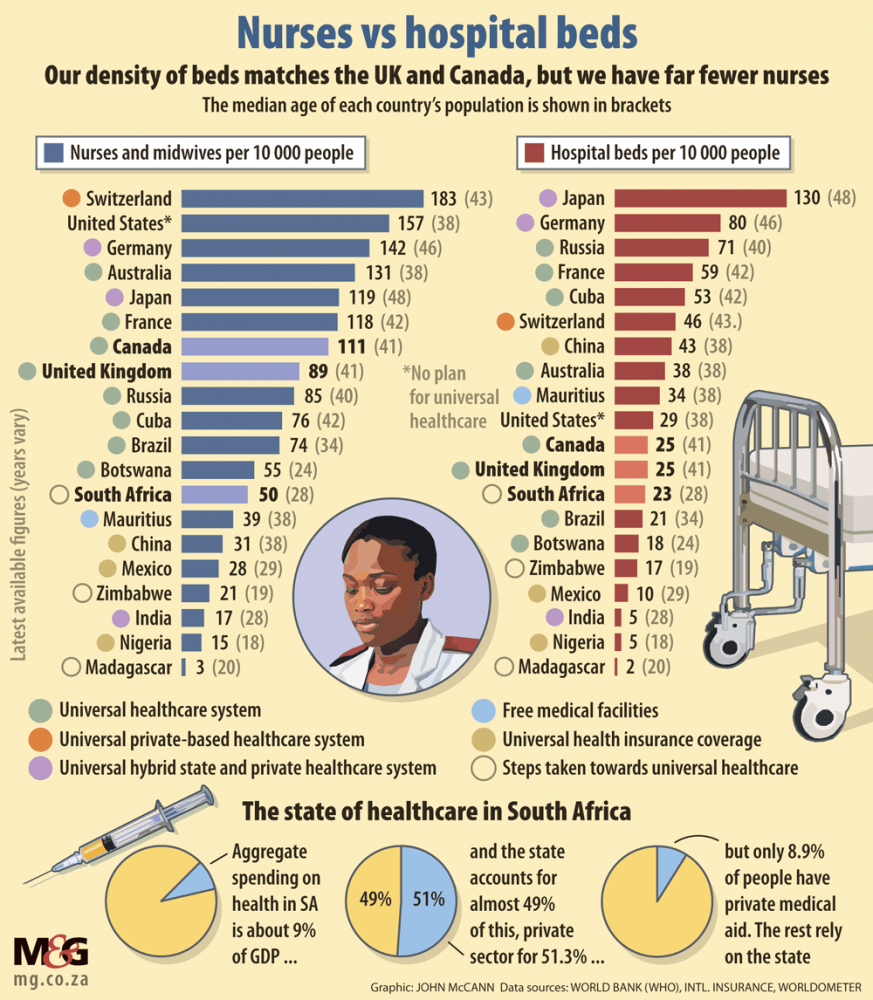
Sixteen percent of the population, 8.9 million people, belong to private medical aids, while the rest are reliant on state healthcare with its well-documented weaknesses. But a study by the Council for Medical Schemes found that 44.5% of members run out of benefits before the end of the year. In 2019, those with private medical aid faced R35.2 billion in out-of-pocket expenditure because their claims exceeded their cover.
A non-negligible percentage of medical scheme subscribers are only covered once they are admitted to hospital. Discovery Health, which dominates the open schemes market with a 57% share, said this went for 14% of its members. Its fastest-growing product is a package that offers more benefits than a so-called hospital plan but does not provide full cover for day-to-day medical care.
It suggests that only a small, monied class have unfettered access to medical care. Or, as one ANC figure advocating for healthcare reform put it: “People think they have medical aid and discover they don’t. And that is our main problem with them [private schemes], they may do many things well but they will deny people care when they need it.”
Once private patients find their benefits are depleted, many forgo further treatment, self-medicate or fall back on to the state’s health facilities, said Nicholas Crisp, the deputy director general of health and the driving force behind the National Health Insurance (NHI).
“We call it dumping,” he said, adding that the state had not calculated the spillover cost because it treated all comers, no questions asked.
The government’s expenditure accounts for just under half of the 8.58% of the GDP that goes towards annual aggregate health spending, while just over 51% is spent in the private sector. Central to Crisp’s thinking, and the NHI bill passed by parliament last week, is the belief that the total sum of nearly R500 billion should be leveraged for the greater good, with the government managing a single fund that pays for all essential treatment.
It is an ideological battlefield where the government distrusts the motives of private medicine, which in turn doubts the state’s ability to deliver, and neither side is wrong.
Opponents are planning to lobby the president not to sign the draft law they see as regressively socialist while proponents say without drastic state intervention, practitioners and private medical schemes will continue to follow the money and serve a fraction of the population.
Busi Mavuso, the chief executive of Business Leadership South Africa (BLSA), said the legislation amounted to a licence to nationalise the private healthcare sector, with dire consequences for the economy.
“What it effectively does is bring in a system in which state provision is the only option and private health provision is effectively closed down, and it does not make sense,” she said.
“You are seeing at the moment, a government that is trying to reverse the monopoly model they have always had. There is this interesting shift in allowing a lot of private participation in a lot of sectors of the economy — electricity, transport, logistics.”
It suggests the state has learnt the limits of its capacity, only for it to ignore these when it comes to healthcare.
Malegapuru Makgoba, the former ombud for health, warned before he retired in May that public health facilities were in decline and most were not fit to implement the NHI.
He added: “It does not mean we should stop trying.”
But Mavuso said with that warning in mind it would be reckless to restrict private medical aid funds to providing cover only for non-essential services.
“So what then becomes of the country if you are taking that option away without giving an alternative, knowing that you don’t have the means, the expertise, the system, the sophisticated models, that you can make this which you are proposing work?” she asked.
Because business interacted directly with multinational firms, it had a responsibility to caution President Cyril Ramaphosa that complete state control of healthcare would alarm foreign investors.
“Maybe we might just get through to them if we actually provide a workable alternative, so if they really value the private sector partnership then they will allow the private sector to look at how we can take this back to the drawing board. It does not have to be signed into law when we know it is not workable.”
She said business believed the United States Affordable Care Act, or Obamacare, which extended private health coverage to some 20 million Americans through state subsidisation, could be explored as a model.
 (John McCann/M&G)
(John McCann/M&G)
But Crisp said the level of inequality in South Africa ruled out any alternative to full state control, including the Bismarck model, which endures in parts of Europe, where citizens pay a fee to fund healthcare provided either by the state or private facilities.
The NHI instead borrows from the Beveridge model, established in England in the 1940s, which makes the state the single purchaser of healthcare funded through taxes.
“We don’t need separate financing mechanisms. And the main reason in this country is that we are the most inequitable society in the world by a long way,” Crisp said.
If specialists, two thirds of whom serve the private sector, and medical schemes could continue operating in parallel to the NHI, Crisp argued, they would focus on patients with deep pockets. “The medical schemes are there to make money, they are not there to provide a service. Even if we said to them they can administer part of the fund, we are not going to allow separate options, we want everybody to have access to the same set of benefits. Massive inequity will never be solved by private sector, free market competition,” he said.
The bill makes provision for the NHI fund to buy services from both the state and the private sector. Patients will register at a primary point of care close to home where treatment will be free and from where they will be referred to hospitals and specialists, if need be.
This, Crisp argues, will put a stop to wanton referrals for expensive investigative procedures or specialist consultations.
“We spend a huge amount of money in the private sector with mothers taking their children to a paediatrician or a dermatologist for things that in the public service a nurse will sort out in five minutes,” said Crisp. “Why would the NHI perpetuate that?”
It is immaterial to him that it was the patient or their medical aid who paid. “It does not matter whose money it is, it is wasting resources that we could have used to care for really sick people in the public sector by sending them to these very same doctors.”
Crisp dismissed the objections that the treasury could not find the money needed for the NHI — R300 billion to R460 billion, according to economists — or that it would rob patients of agency because they could not obtain treatment without referral.
The implementation of the NHI will “start in a small way” with the first phase due to run until 2026 to cater for mothers and children. The second phase will run until 2028 and see the introduction of taxes that will fund the scheme. Full implementation will possibly take decades..
Regarding elective treatments, Crisp said: “If there is no clinical indication [for it], and you choose something, then you pay for it.”
Section six of the bill stipulates that citizens could only access complementary care through voluntary medical insurance or pay for it out of their pockets, which is already the case. He said this would include vanity orthodontics and “fancy reading glasses”, but a list will be published in a schedule determined by a committee to be appointed in due course.
Parliamentary legal advisers have said it is less clear what would happen if a patient wished to consult a specialist for illness though their primary doctor did not deem it necessary. The law requires “absolute and unwavering adherence to referral pathways by both providers and patients”, they noted, and allows no flexibility for when failure to follow that pathway is reasonable. A reduction in access to treatment could trigger a challenge in terms of section 27 of the Constitution.
Bandile Masuku, the former Gauteng MEC for health, said opposition to the NHI and the power the bill gives to the health minister was informed by years of state capture and would all but disappear if the government would allow a multi-payer system where citizens were free to access private facilities through state subsidisation. It would help if the government could, before the bill was signed, approach private institutions to negotiate tariffs to clear backlogs in the public system, and bring clinics to function optimally.
“It would change the whole narrative and lessen resistance if we demonstrate that it can be done, and it is not about ideology but we can meet in the middle ground,” Masuku said.
There should be no illusion that there would ever be enough funding to roll out what passes for private healthcare treatment to the population at large.
“In the current form, the way we are delivering healthcare both in the public and private system is unaffordable, whether it is the NHI or Discovery. We need to move to investing in primary healthcare, with a focus on prevention.”
Masuku warned that without communicating this paradigm shift, the ANC was creating expectations ahead of next year’s national election that it would eventually disappoint.
Mavuso said something similar.
“You can’t think this is a signalling exercise to hopefully win over the electorate and they are going to forget about it. They are going to remember because they want you to deliver what you promised.”