Christian devotees take part in a prayer mass at St. Joseph's Cathedral on the eve of Good Friday, in Allahabad on April 1, 2021. (Photo by SANJAY KANOJIA / AFP)
With the news of a new Covid-19 variant circulating in India possibly having made it through South African ports of entry, scientists say it is too soon for citizens to panic.
Although no cases of B.1.617 — the variant blazing through India — have been reported in South Africa, as stated by the National Institute for Communicable Diseases, specialists have started investigating it.
In its weekly epidemiology update, the World Health Organisation (WHO) reported that the B.1.617 was a variant of interest and might be responsible for the surge in Covid-19 cases in India.
With a 52% increase, India has, since the pandemic started, reported more than 2.2-million cases. On one day this week, India had more than 357 000 new cases. In the first year of the pandemic, India recorded about 10-million cases. The second 10-million cases were reported in the past five months, especially in April.
According to the WHO, further studies into the phenotypic effects of this and other variants must be investigated. These include epidemiological characteristics such as transmissibility, severity, reinfection risk, and its effect on countermeasures.
Existing data show that the B.1.617 variant has now been found in more than 30 other countries in Europe, Asia and North America.
Professor Carolyn Williamson, from the Medical Virology Division at the University of Cape Town, said travellers from India were being screened for the variant.
“It has not yet been detected in South Africa. However, there is an ongoing investigation by the Network for Genomics Surveillance in South Africa, where we are screening travellers from India to determine if this variant is being introduced.”
The ministerial advisory committee apparently met on Thursday to discuss recent developments regarding B.1.617.
Will vaccines be effective?
Professor Ameena Goga, director of the South African Medical Research Council’s HIV Prevention Research Unit, says there is not enough information to tell whether the existing vaccines would be effective against B.1.617, but they have been proven to have high efficacy rates.
Professor Francois Venter, head of research group Ezintsha at the University of the Witwatersrand, said: “It is interesting but likely that all vaccines will have breakthrough infections. We have seen protection from severe disease with all the accepted vaccines, which is the most important endpoint.
“Providing what we call sterilising immunity [stopping infection] isn’t nearly as important as stopping disease and death.”
Williamson says existing evidence on B.1.617 does not indicate whether it will be worse than the 501Y.V2 that emerged in South Africa.
“Like the 501Y.V2, there are a few mutations that are of concern that may increase infectivity and have been associated with escape from neutralising antibodies that may result in vaccines being less effective. However, there is no evidence currently to suggest it will be worse than 501Y.V2.”
 (John McCann/M&G)
(John McCann/M&G)
Is the variant a concern?
Most countries have closed their borders to countries where mutations of Covid-19 resulted in new variants, such as South Africa and India.
This was done to prevent importing these variants, but South Africa has kept its borders open to India.
In December, countries such as Switzerland, Turkey, Germany, and Israel temporarily closed their borders to anyone from South Africa or banned flights from the country and Britain.
The minister of health, Dr Zweli Mkhize, released a statement about the possibility of “importation variant concern”.
This came after three air travellers from India arrived in the country last month. The first passenger fell ill and is isolating at a health facility. The other two passengers are asymptomatic and also in isolation.
A vessel from India that berthed at the Maydon Harbour in Durban has seen 14 of the 21 crew testing positive for Covid-19. The results of a person who died aboard have not yet been released.
Another traveller from India was found to have contracted the 501Y.V2 variant at the Stellenbosch University after being suspected of having the B.1.617 variant.
Without evidence that the variant is responsible for the surge of the number of cases in India and with data not showing that the B.1.617 is worse in terms of transmissibility and antibody escape than the 501Y.V2 dominating in South Africa, Williamson said there was “no need to panic” but “as a country, we need to be vigilant around the emergence of new variants and to protect ourselves and our contacts from infection … We should, however, continue to monitor and learn more about this [B.1.617], and other variants, that are emerging around the world.”
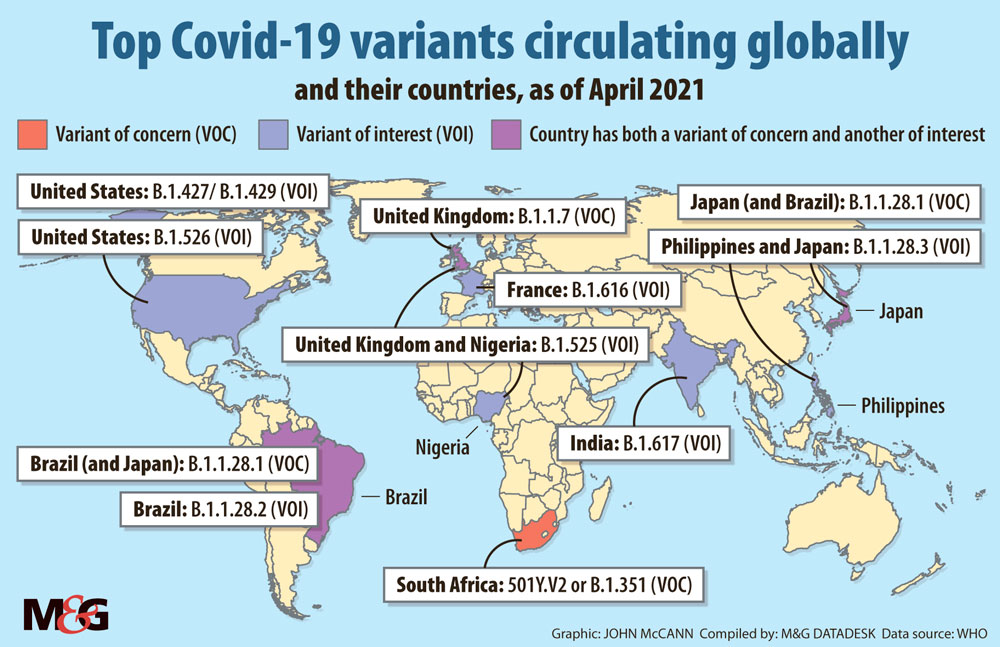
How many variants globally?
The B.1.617 is one of 10 variants that the WHO has listed as either variants of interest or concern. As of 27 April, the 501Y.V2 is one of three variants of concern.
Since August last year, the 501Y.V2 had remained dominant in the country; it was found to have been transmissible by 53% more than previous variants. It resulted in a surge in the number of Covid-19 cases, especially during the festive season months in the coastal provinces of KwaZulu-Natal and the Western Cape.
Out of the vaccines tested for efficacy and effectiveness against the 501Y.V2 variant, the AstraZeneca vaccine, which had previously fared high with an efficacy rate of up to 75%, was found to provide only 22% protection against mild to moderate infection caused by 501Y.V2.
AstraZeneca was withdrawn from the government’s vaccine rollout plans and replaced by the Janssen vaccine from Johnson & Johnson (J&J) through the Sisonke phase 3B trial, which has seen just under 400 000 health workers receiving the single-dose vaccine.
The J&J vaccine has been granted registration with conditions by the South African Health Products Regulatory Authority for its use in the implementation study. It offers up to 57% protection from moderate to severe illness.
It has also been shown to reduce symptoms by up to 67% among the study participants, effectively preventing severe disease and protecting participants from being admitted to hospital and death.